58
|
CERECDOCTORS.COM
|
QUARTER 3
|
2015
| | |
D I S C U S S I O N F O R U M
cements, while beingmarketed as radiopaque, are anything but.
There’s a guy in Europe (don’t remember name) doing research
on cement retained around implants. Basically any restoration
extending beyond 1 mm from implant platform (1 mm of emer-
gence profile) will have cement after clean up. We simply can’t
get our instruments around the convex restoration to the base to
remove it all (a great argument for screw-retained restorations).
Hopefully I’ve done an adequate job relaying his research and, if
I’mwrong, someone please correct me.
ROSS ENFINGER
Implants are more susceptible to bone loss due to
cement sepsis because of the difference in physi-
ology of soft tissue attachment around implants versus the
cementumof natural teeth. Implants have aweaker hemidesmo-
somal attachment, and the fibers don’t run in the same direction
as seen on natural teeth, both of which make themmore friable
and susceptible to tearing forces like cement excess.
ROSS ENFINGER
Well, Steven beat me to it and explained it much
more thoroughly. Well done!
JIM STEIN
Chalk up one for a good guess.
BRIAN CHAN
The problem with cement sepsis should really
be a moot point if using e.max abutment blocks/
custom abutments. Since we are able to control the depth of
the margins, seems like cement sepsis shouldn’t be an issue
like this particular case because the margin won’t be so deep.
I tried that “cement on an analog, then transfer into the
mouth.” It did not work well as there was so little cement over-
flow that I wasn’t sure if I cleaned everything up or not.
DMITRI RUZANOV
Gregory is spot-on when mentioning bone turn-
over issue.
Look at the regenerated ridge, look at the distal implant
site. Compare to the mesial implant site. See the difference in
color; the distal site is whitish and doesn’t look like bleeding.
That means the distal site never turned into vital bone.
Yes, you’ll get the implant in. But it is just a screw in dead
bone. When subjected to loading, this “bone” gets replaced
by granulation tissue. And you don’t even need any cement
sepsis on these cases.
JEFF JOHNSON
Great thread and thoughts.
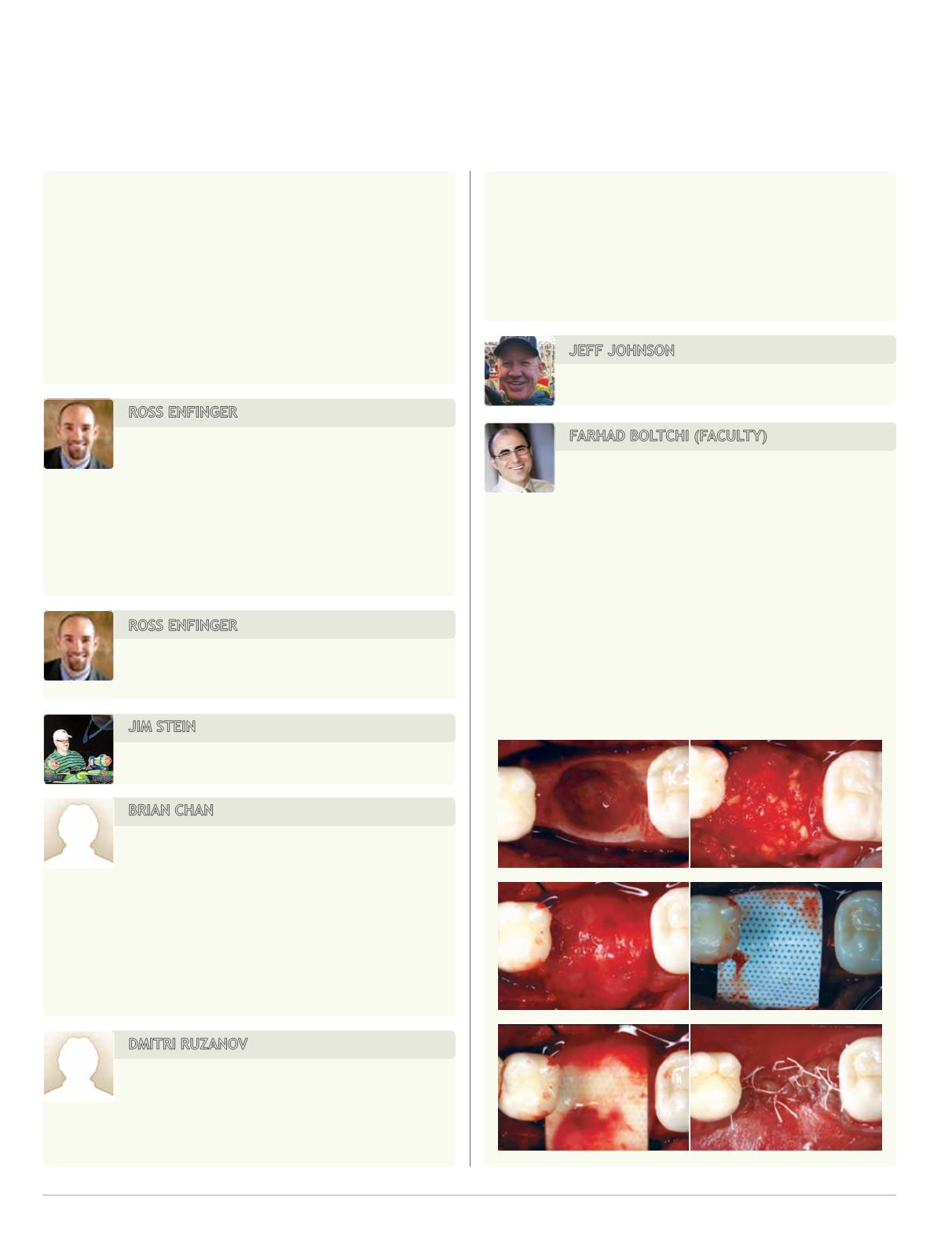
FARHAD BOLTCHI (FACULTY)
I am sorry Dmitri, but this is utter nonsense unless
you are talking about a block allograft.
I have been doing this for 21 years now, and I have had an
implant failure rate of 0.2 percent (of the patients I have been
able to follow up). Every single time I have been able to iden-
tify a cause for the failure, e.g. cement sepsis, occlusal overload,
smoking. I have generally not seen any difference between
regenerated bone and host bone in this regard except that
regenerated bone in its early stages seems to break down easier
than the host bone when subjected to one of these causes. This
has also been proven over and over in numerous studies.
Here is the rest of this case. Explanation will follow later.


