56
|
CERECDOCTORS.COM
|
QUARTER 3
|
2015
| | |
D I S C U S S I O N F O R U M
ANTHONY KRAFT
But if itwas theparticulate,wouldn’t youexpect tooth
#20 to be in the same situation? I’m thinking para-
function, occlusal issue, restorative or a combination of these?
Farhad, when prepping for implant placement, did the
bone seem viable — good bleeding, etc.? Thanks for sharing;
obviously a bummer.
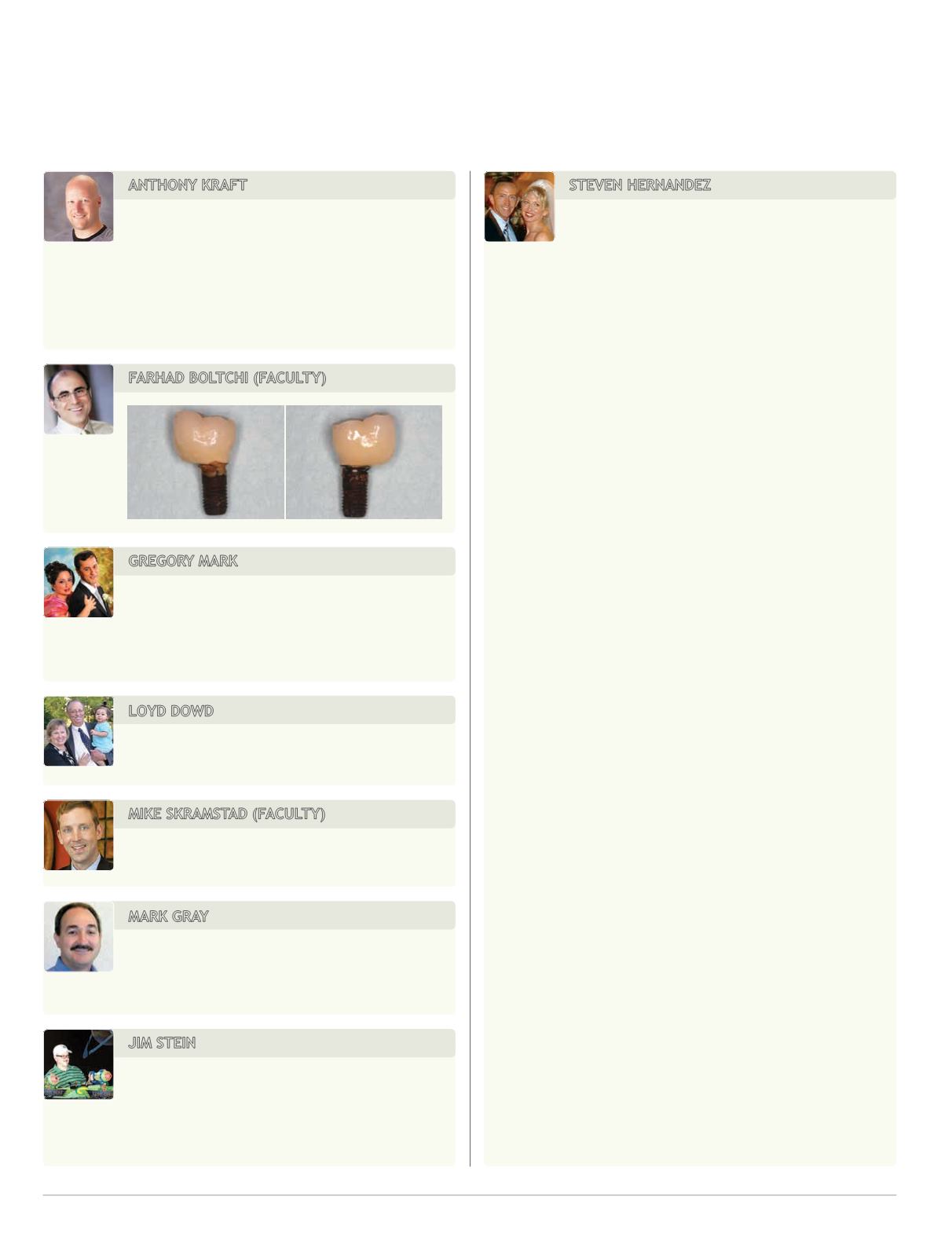
FARHAD BOLTCHI (FACULTY)
GREGORY MARK
Farhad: Why cement only resorb the bone only
with implants but not with teeth? Sometimes we
see good clinical pictures on X-ray and clinically, maybe patient
already had a pocket and cement was just a secondary cause?
LOYD DOWD
Beautiful graft result. Wish all of mine turned out
that good.
MIKE SKRAMSTAD (FACULTY)
This looked like a cement sepsis case due to poor
contours of the restoration.
MARK GRAY
Another indication would be the length of time it
took to happen: 2008 to 2013. Seems if cement is
involved, it takes about five years to show up.
JIM STEIN
I would hazard a guess that the cement disrupts
the gingival attachment on the implant allowing
bacterial infiltration whereas the excess cement on a crown
acts more like calculus as a mechanical irritant.
STEVEN HERNANDEZ
Was at an implant course this past weekend and
heard Chandur Wadhwani speak on this very
subject. AMAZING lecture. Think of it this way: When we
cement crowns on teeth as we have for many years, we don’t
see this. Why? The attachment apparatus. Remember from
dental school howmany fibers there were; horizontal, oblique,
etc? The same doesn’t exist with implants. The fibers basically
encircle the implant. And the attachment is a hemidesmosome;
the weakest ‘attachment’ in the body.
Now here’s where the lecture got interesting. He asked
dentists how they cemented crowns to teeth; did they fill the
entire intaglio ... just put cement around the rim ... paint it inside
with a brush? There’s no ‘standard.’ His research suggested
using cement in one of two ways:
1. Apply Teflon tape to implant analog. Fill crown with
cement, seat on analog, remove crown, deliver in mouth.
2. Spread bead of cement on the intaglio in a circle just inside
the margin.
To better evaluate dental cement, he contacted a large
research company that tests fluids. They began by asking him if
the cement we use in dentistry is Newtonian or non-Newtonian.
He immediately understood that we, as a profession, don’t know
much about the material we use. So, Newtonian fluids are like
water: theyfill/take theshapeof theircontainer.Non-Newtonian
is like ketchup. It’s ‘solid’ in its container but takes on Newto-
nian (water) properties when pressure is applied (like when
you squeeze the ketchup bottle and it squirts out like water). So
much research was done with regards to implant abutments,
crowns, seating force, seating time, where the cement is placed,
etc. Here’s the bottom line.
Cement placed inside crown at the occlusal surface
(deepest part of crown) is the worst place.
Seating a crown ‘too fast’ (more research needed to know
“ideal” seating speed) is bad.Why? Becausewhen seatedquickly
and force is applied, our cement takes onproperties ofwater and
is basically injected around the implant. The fibers aren’t strong
enough to stop the cement from penetrating. This is not b/c the
implant isn’t integrated; rather the trabeculae of the bone itself.
When pressed for a cement he recommends, he said ZONE.
He and Tom Wilson also looked at the various cements we
dentists use to cement implant crowns andwhat thicknesses are
needed before they appear onX-rays. Some of themore popular


